
Depression is a system-performance issue
The untreated depression gap is avoidable service pressure, lost productivity and inequality — not only a mental-health prevalence problem. Live NHS Talking Therapies activity is shown below.
Referrals received vs accessing services — England, monthly Open · NHS live
Prevalence
A persistent need pool: prevalence has not returned to pre-pandemic levels while service capacity is constrained.
Access & workforce
A standing gap between referrals received and people entering treatment — workforce-limited, not demand-limited.
Medication limits
Non-response and tolerability leave a sizeable cohort needing a drug-free, scalable option.
Inequality
Need is concentrated in high-deprivation areas where access and recovery lag the England average.
BioVie Beam — a pathway-ready tDCS intervention
A non-invasive, drug-free, reusable transcranial direct-current stimulation (tDCS) headset designed for supervised home use, deployed B2B through health systems — not a consumer wellness gadget.
Patient flow
Pathway fit: primary care, NHS Talking Therapies step 2/3, and specialist mental health — as an adjunct or waiting-list option under clinical oversight.
Every headline traces from data to conclusion
The tool runs on an open-data spine — live NHS Talking Therapies statistics — with explicit modelled assumptions you control. Every figure carries a source label; local data improves precision when commissioners share it.
Open
Published NHS / ONS / NIMH statistics, refreshed automatically from the live source each month.
Evidence Regulatory
Peer-reviewed trials and official FDA records — cited, dated, never paraphrased.
Modelled
Editable scenario assumptions with stated defaults and ranges. Marked illustrative until validated.
Local TBC
ICB-supplied costs, pathway data and pilot results — placeholders today, replacing estimates as they arrive.
Quantify the national opportunity in courses, not pounds
Before localising, the scale of the corridor: real referral volumes, the standing access gap, and what 1–10% penetration of annual referrals would mean in treatment courses.
Penetration scenarios Modelled Illustrative
Scenario units are annual BioVie Beam courses as a share of observed annual referrals. They are demand corridors for planning — not forecasts, and deliberately not converted to revenue in this commissioner view.
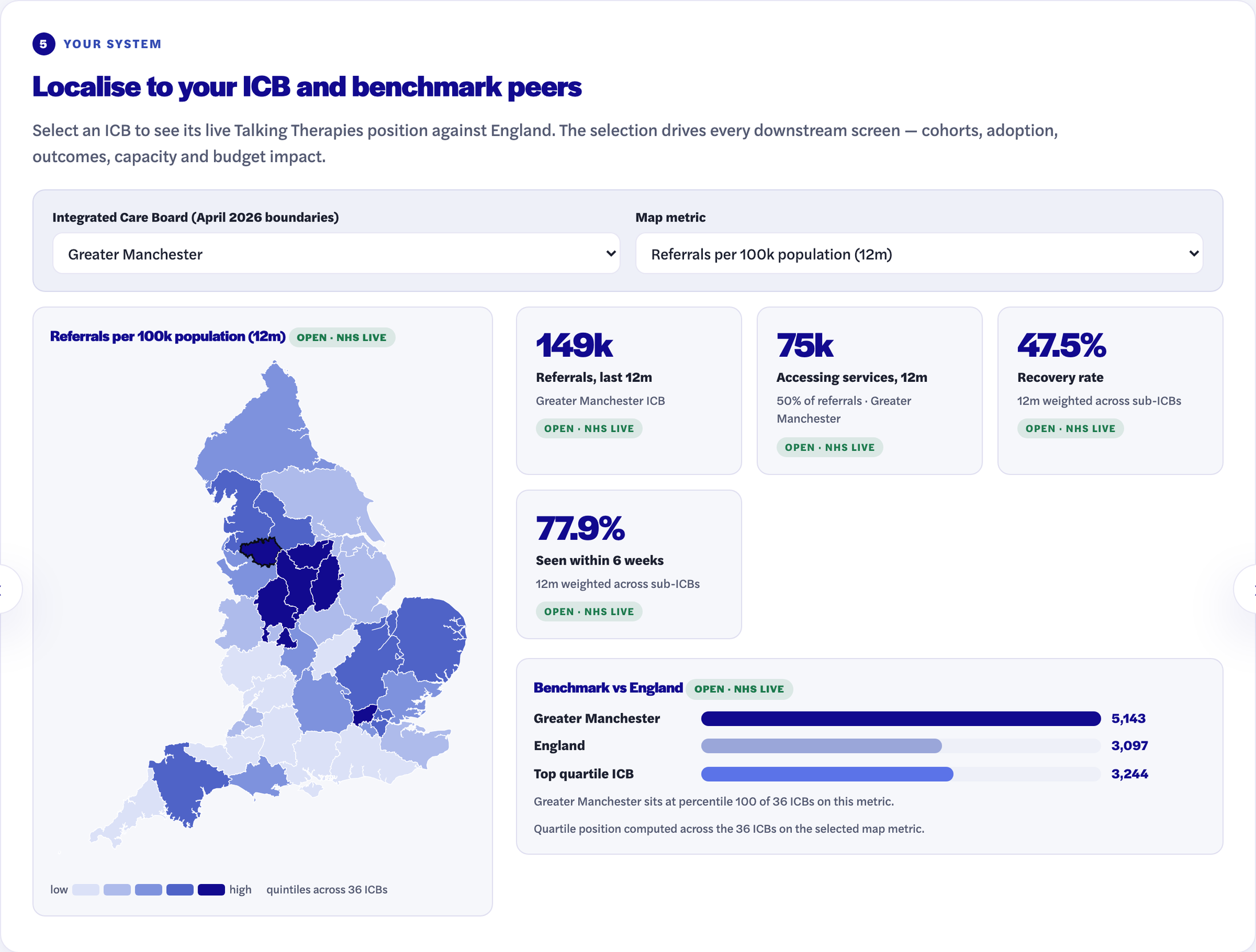
Localise to your ICB and benchmark peers
Select an ICB to see its live Talking Therapies position against England. The selection drives every downstream screen — cohorts, adoption, outcomes, capacity and budget impact.
Referrals per 100k Open · NHS live
Benchmark vs England Open · NHS live
Make the eligible cohorts visible
From the live local referral base to a clinically plausible, pilot-ready cohort. Suitability and prioritisation rates are editable assumptions that need clinical sign-off — they are deliberately conservative defaults.
Suitability reflects pathway position (waiting / step 2-3), medication intolerance or non-response, relapse prevention and exclusions. Local TBC Local case-finding data replaces these estimates when shared.
Expose the adoption conversion gap
The opportunity — clinical and operational — is the gap between eligible patients and completed courses. The gap decomposes into identification, prescribing, supply, adherence and follow-up so effort goes where it matters.
Convert adoption into outcomes commissioners recognise
Completed courses become response and remission using published category evidence, with explicit sensitivity. These are comparator-device anchors — BioVie-specific evidence is generated through the pilot programme.
Recast treatment as released system capacity
Why this matters to NHS leaders beyond the device budget: completed home-based courses can displace therapy appointments, releasing slots and clinician time into the waiting list.
Released capacity is presented as operational value. It is only cash-releasing if a commissioner chooses to take it as cost; otherwise it shortens waits. Local TBC Local staffing and waiting-list data sharpen this materially.
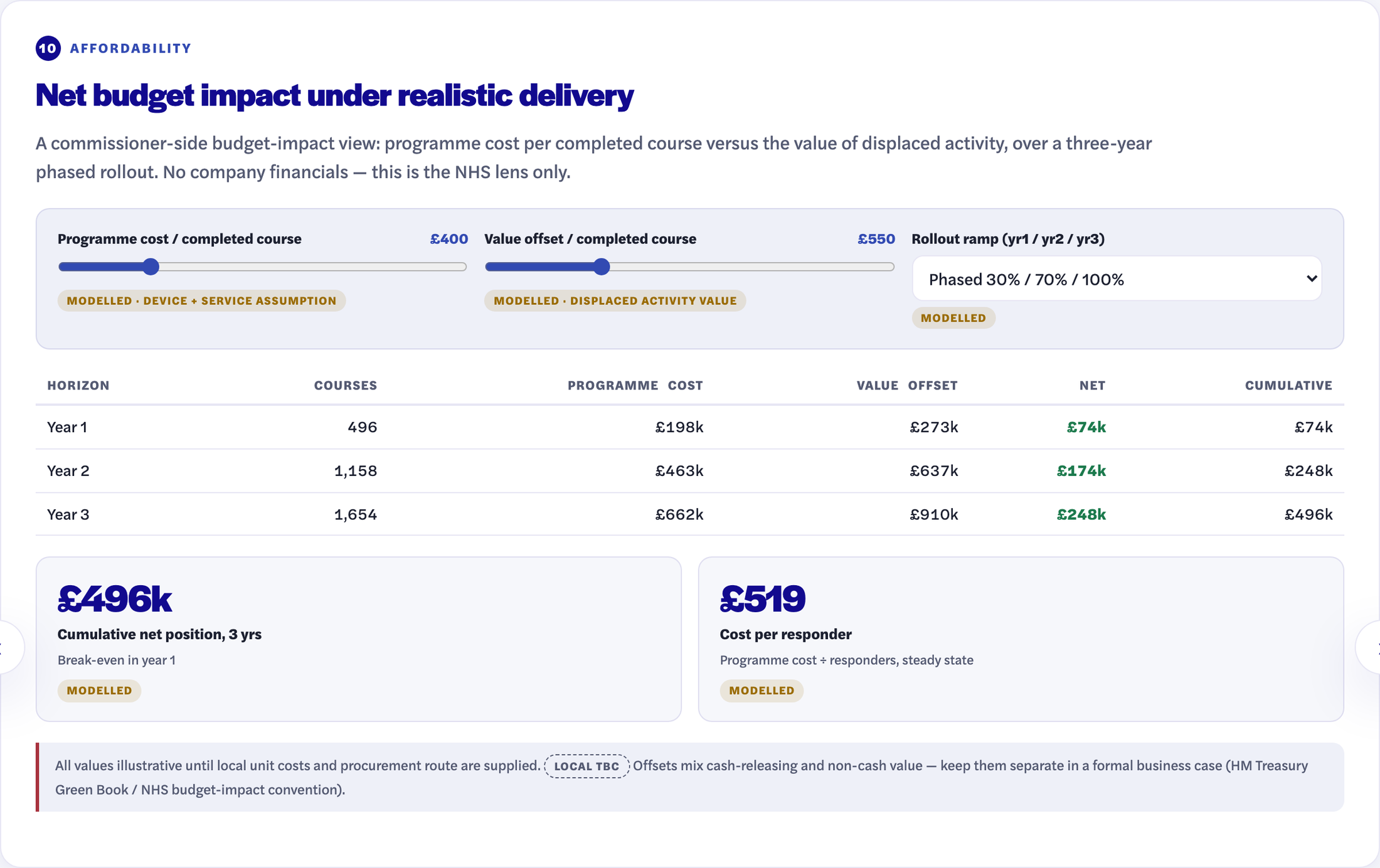
Net budget impact under realistic delivery
A commissioner-side budget-impact view: programme cost per completed course versus the value of displaced activity, over a three-year phased rollout. No company financials — this is the NHS lens only.
All values illustrative until local unit costs and procurement route are supplied. Local TBC Offsets mix cash-releasing and non-cash value — keep them separate in a formal business case (HM Treasury Green Book / NHS budget-impact convention).
The category is validated; BioVie executes its own path
Recent FDA approval of an at-home tDCS comparator validates the category — home use, prescription oversight, MDD indication — and de-risks the sector. It does not approve BioVie Beam: BioVie still requires its own evidence and submissions.
FDA PMA P230024 — Flow FL-100 Regulatory · FDA
Premarket approval, decision 8 December 2025: the first at-home brain-stimulation device for depression. Indication (FDA wording): treatment of moderate to severe major depressive disorder in adults, as monotherapy or adjunctive therapy, in patients not considered treatment refractory to medication.
Peer-reviewed trial evidence Evidence
Home-based tDCS for major depressive disorder: 10-week randomised controlled trial reporting efficacy, acceptability and safety (Nature Medicine, 2024). Category evidence base of 9,000+ tDCS publications cited in BioVie materials Internal.
US market context Open · NIMH
21.0m US adults had a major depressive episode in 2021 (8.3% of adults, NIMH/NSDUH). Comparator US launch was reported with a $500–$800 price corridor News · Reuters — context for category economics, not BioVie pricing.
What it means for commissioners Inference
The regulatory question has moved from “is at-home tDCS approvable?” to “can BioVie execute a differentiated, compliant evidence and access pathway?” Category risk is reduced; product-specific execution risk remains and is addressed through the pilot and evidence plan (screen 12).
Required caveat: comparator approval validates the category only. BioVie Beam is not FDA-approved, not CE-marked Class IIa today (target), and requires its own clinical evidence and regulatory submissions.
Decision, not dashboard
What a system can do next, and the full register of every assumption and source behind the numbers above — so the case is scrutinise-able and exportable.
1 · Pilot
Resource first-wave pilot sites in the selected ICB; agree the eligible-cohort definition with clinical leads.
Local TBC2 · Measure
Capture starts, completions, adherence, outcomes and drop-off reasons — pilot data replaces the modelled defaults on screens 6–10.
Modelled → real3 · Commission
Convert the validated budget-impact case into procurement and reimbursement routes; build the next ICB wave from peer benchmarks.
Internal planAssumptions register Live — reflects current slider state
Source register
| Source | Type | Used for |
|---|---|---|
| NHS Talking Therapies Monthly Statistics | Open | Referrals, access, waits, recovery — England & ICB (live, auto-refreshed) |
| ONS — depression in adults | Open | 17% prevalence anchor (PHQ-8, 2021) |
| UK Parliament PAC report | Open | £12bn NHS mental-health spend, 2021/22 |
| Nuffield Trust — IAPT/TT programme | Open | 1.9m access ambition context |
| FDA PMA P230024 + SSED | Regulatory | Comparator approval, indication wording, evidence package |
| Nature Medicine 2024 | Evidence | Home-based tDCS RCT — outcome anchors |
| NIMH major depression statistics | Open | US 21.0m / 8.3% MDE anchors (2021) |
| Flow Neuroscience public materials | Company | 77% / 57% comparator real-world anchors |
| BioVie product & programme documents | Internal | Product features, regulatory targets, pilot plan |
| ICB / provider local inputs · pilot CRM | Local TBC | Local costs, pathway data, pilot outcomes — future |